
We would like to thank our friends at Save Ellis Island for their contributions to this exhibit.









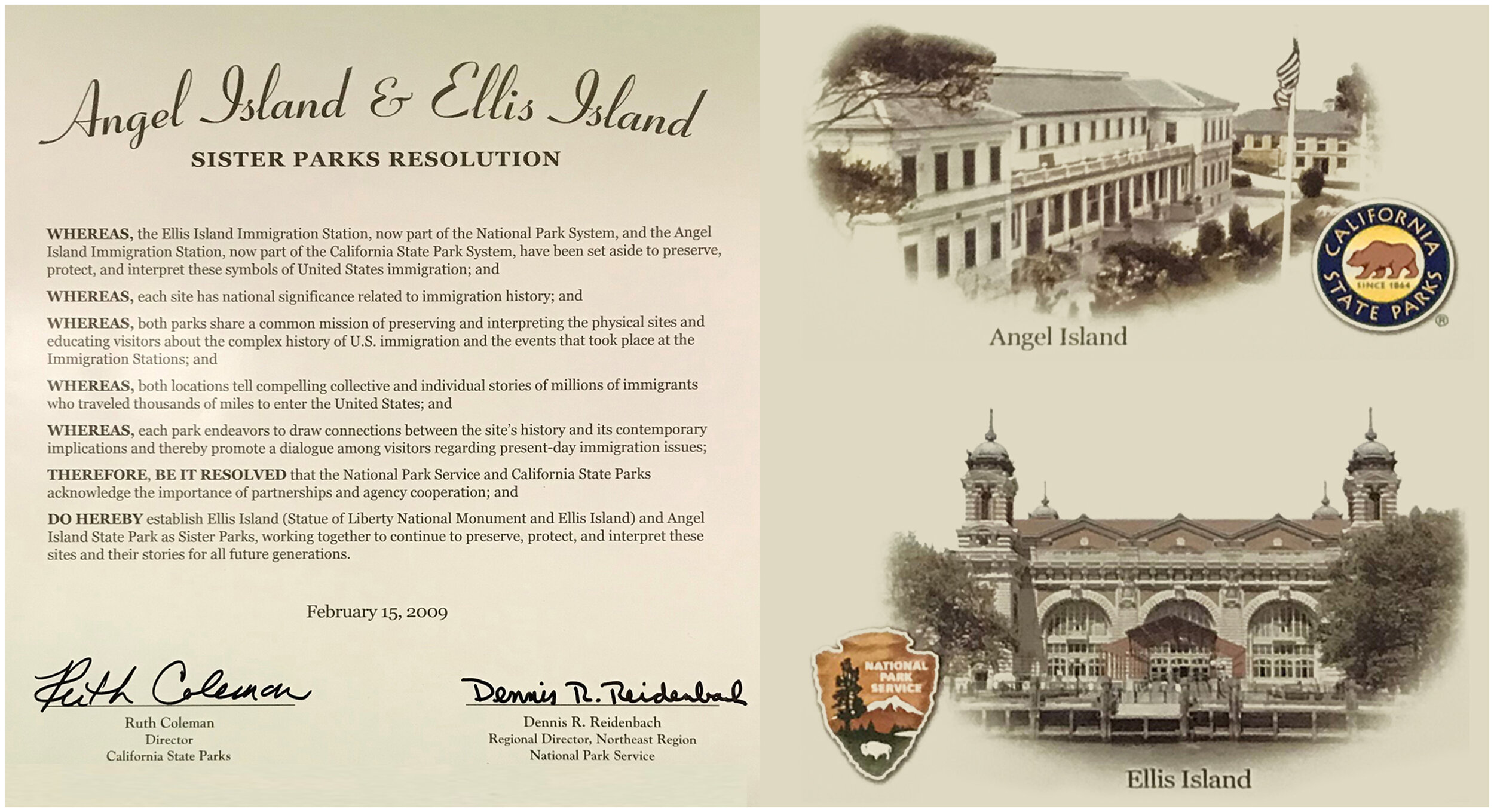
The U.S. Public Health Service was responsible for the inspection and/or treatment of over 13 million immigrants at Ellis Island and Angel Island – the two largest immigration ports on either coast. Ellis Island officially opened in 1892, so when Angel Island was announced to open in 1910, the San Francisco Call playfully nicknamed it “San Francisco’s New Ellis Island” due to the similarities it shared with its New York predecessor. Although there were similarities, they also had dramatic differences. Between 1910 and 1940, Ellis Island rejected only 6% of the immigrants arriving in New York Harbor. Meanwhile, during that same period, Angel Island rejected as many as 33% of the immigrants arriving in San Francisco Bay.
The role of the U.S. Public Health Service existed independently from U.S. Immigration Services. The PHS defined its mission rather narrowly —preventing the entrance of disease to the nation — but PHS officers interpreted their job more broadly. In their eyes, the goal was to prevent the entrance of undesirable people — those “who would not make good citizens.” In the context of industrial-era America, immigrants who would wear out prematurely, requiring care and maintenance rather than supplying manpower, would not make “good” citizens.
The diagnostic protocol emphasized the physician’s “gaze,” demonstrating the conviction that disease was written on the body. Dr. Albert Nute, while stationed in Boston, argued that “almost no grave organic disease can have a hold on an individual without stamping some evidence of its presence upon the appearance of the patient evident to the eye or hand of the trained observer.”
SIX-SECOND SPECIALISTS / Ellis Island
On Ellis Island, new arrivals formed a long line that wound its way up the stairs and into the Registry Room. U.S. Public Health Service doctors stationed at the stairs sometimes had only six seconds to scan each immigrant during the line inspection to detect those who should be held for a more thorough medical examination.
If a doctor found any indication of disease, he marked the immigrant’s clothing with chalk: L for lameness, E for eyes, H for heart, Ct for trachoma, Pg for pregnant, X for mental illness, etc.
Immigrants marked with a chalked letter during the line inspection were led to examination rooms. There, a doctor would check them for the ailment indicated by the chalk mark and give them a quick physical. Many immigrants had to be sent to the Ellis Island hospital for observation and care.
Image: Ellis Island, New York, Circa 1910-1920. Courtesy of National Archives
INSPECTIONS AND DETAINMENT / Angel Island
Physicians on Angel Island looked for many of the same diseases as their counterparts on Ellis Island, such as trachoma, but they were particularly interested in the common parasites carried by Chinese and other Asians.
Diseases such as uncinariasis (hookworm), filariasis, and clonorchiasis (liver fluke) were more prevalent among Asians. This led to Chinese immigrants being detained if any of these parasitic diseases were detected.
Upon completion of their medical treatment, immigrants were returned to their dormitories to await a hearing on their applications. In many cases, the wait for a hearing stretched into weeks or months because of the backlog and the extensive investigations that Chinese cases entailed.
Image: Angel Island, California, 1923. Courtesy of the National Library of Medicine
By 1903, the U.S. Public Health Service had codified diseases into two major categories: “Class A” loathsome or dangerous contagious diseases and “Class B” diseases and conditions that would render an immigrant “likely to become a public charge.” A subset of Class A conditions included mental conditions such as insanity and epilepsy.
MENTAL TESTING / Ellis Island
By 1917, immigration laws prohibited the admission of all aliens diagnosed as suffering from any mental impairment. The immigrant population’s wide variety of educational and cultural backgrounds, however, made assessing individual intelligence extremely difficult.
To screen new arrivals, Ellis Island doctors used standard intelligence tests as well as tests they developed themselves in an attempt to deal with these cultural differences.
In addition to using standard tests, doctors often used puzzles and mimicry tests because they did not have to be explained to the immigrant through an interpreter; nor did an immigrant have to know how to read or write in order to solve them. Other puzzles that tested spacial relations and problem solving were used to check immigrants’ mental capacity.
Image: Ellis Island, New York, 2019. Courtesy of Russell Nauman
IDENTIFYING PUBLIC CHARGES / Angel Island
On Angel Island, doctors dubbed germs “the most democratic creatures in the world.” They believed they could use science as a tool to screen immigrants objectively, regardless of skin color or social status. However, not all immigrants underwent the same types of exams, and certain groups were subject to additional scrutiny.
Immigrants were also evaluated based on their perceived fitness and wealth. They were excluded if they were labeled a “likely public charge” (LPC), which meant they were considered to be a current or future economic burden to the country.
Some immigrants were ruled LPCs because of “physical defects.” Single women were often seen as “moral risks” and then deemed LPCs as a result. In many cases, LPCs were admitted into the U.S. if they could post a $500 public charge bond. Those who could not afford to pay faced deportation.
Image: Record of Aliens Held for Special Inquiry, 1914. Courtesy of National Archives and Ancestry.com
On the East Coast, medical exams served more of a processing than exclusionary function for European immigrants. Non-Europeans faced more considerable medical obstacles to entry at Angel Island. Asians immigrants arriving in San Francisco endured an invasive physical exam in addition to routine laboratory testing for parasitic infection, which required detention at Angel Island for days, weeks, or longer. “Disease,” public health officials argued, “was not so easily read in the inscrutable Asians, particularly the Chinese.”
HOSPITAL COMPLEX / Ellis Island
By 1911, more than 15 buildings on the island were devoted to medical care. The U.S. Public Health Service operated a 275-bed hospital and contagious disease wards with 450 beds. There were laboratories, operating rooms, an x-ray plan, a psychiatric ward, and a morgue.
A separate medical complex for the treatment of contagious diseases opened behind the hospital buildings in 1911.
The staff of doctors dealt with every kind of medical impairment, from slight injuries to rare tropical diseases. Though death was a far more frequent occurrence, births too were part of the hospital routine. Over 355 babies were born on Ellis Island. One observer said, “It is at once a maternity ward and an insane asylum.”
Image: Ellis Island, New York, 2019. Courtesy of Russell Nauman
TWO DISTINCT BUILDINGS / Angel Island
When the hospital was built in 1909, there were two separate entrances for immigrants: European and Non-European. This was done to help prevent “disease transmission between the races.” At its peak capacity, the hospital could hold 60 to 80 beds. Most of the first floor was designed for administrative use, but some other areas included segregated dining rooms, bedrooms for medical staff, and a morgue.
The segregated design of the hospital was intended to create “practically two distinct buildings” to separate Asians and Europeans.
The hospital had a small ward for treating highly contagious diseases. During the two meningitis outbreaks on Angel Island (1914 and 1921), tents were erected behind the building to accommodate infected patients.
Image: Angel Island, California, 2020. Courtesy of Russell Nauman
Since their closure, both Ellis Island and Angel Island have been transformed into historical sites that focus on our nation’s immigration story. The Public Health Service hospital serves an important role in understanding what many immigrants faced when they arrived at America’s door. By interpreting these spaces for the public, we can begin to understand the connection between immigration, policy, and public health.
FUTURE OF THE HOSPITAL COMPLEX / Ellis Island
Despite the historic significance of Ellis Island, the entire island was deemed surplus U.S. government property in 1954 and was abandoned. Following the Supreme Court ruling in 1999 giving New Jersey sovereignty for 22.5 acres of Ellis Island, Save Ellis Island was formed to raise the funds needed to rehabilitate and repurpose twenty-nine historic buildings of the Immigrant Hospital Complex.
Save Ellis Island’s objective, in cooperation with the National Park Service, is to restore the “Southside” of Ellis Island in its entirety and create a viable, sustainable re-use that offers the maximum public benefit that is reflective of Ellis Island’s importance in the history of the United States.
Image: Ellis Island, New York, 2019. Courtesy of Russell Nauman
THE ANGEL ISLAND IMMIGRATION MUSEUM / Angel Island
After the hospital closed in 1946, the building fell into disrepair. The Angel Island Immigration Station Foundation, in collaboration with California State Parks, embarked on a renovation project that began in 2005 and was completed in 2020.
The result of these efforts became the Angel Island Immigration Museum.
The goal of the new museum is to represent the stories of Pacific Coast immigrants thoughtfully and to make personal stories readily accessible to visitors at both the site and online. (read more…)
Image: Angel Island, California, 2020. Courtesy of Russell Nauman
We would like to thank our friends at Save Ellis Island for their contributions to this exhibit.
